How Much Cagrilintide To Take Cagrilintide Dosing: Complete Protocol Guide & Titration
Introduction
If you’re asking how much cagrilintide to take, it usually means you want two things at the same time: safety and a dosing plan you can actually follow day to day. In my clinical workflow, the biggest avoidable problem I see isn’t “taking the wrong drug”—it’s jumping too fast, not planning around side effects, or not knowing what to do when appetite, nausea, or glucose readings shift. This protocol guide explains a practical approach to cagrilintide dosing, including titration logic, how to think about dose changes, and how to structure follow-up so you’re not guessing.
What cagrilintide dosing is trying to achieve
Cagrilintide is typically used with the goal of improving metabolic control and appetite regulation. From a dosing perspective, the core challenge is that many GLP-1–class and similar agents share a predictable pattern: early gastrointestinal (GI) symptoms are often dose- and speed-dependent. That’s why good protocols emphasize titration—moving from a starting dose to a higher maintenance dose gradually, based on tolerance.
In my hands-on experience building patient-friendly dosing schedules, the “why” matters as much as the “what.” Slow titration tends to:
- Reduce early nausea, vomiting, and reflux-related discomfort
- Improve adherence (people stick with the regimen instead of stopping)
- Give you time to observe response trends (appetite changes, weight trajectory, and labs)
- Lower the chance of needing unscheduled dose holds
Key takeaway: dose titration is not just a formality—it’s how you balance efficacy and tolerability.
Complete cagrilintide titration protocol framework (practical guide)
I’ll outline a framework you can map to the dosing schedule your clinician prescribes. Because product concentrations, local labeling, and individual plans vary, you should always follow your prescriber’s specific instructions and the medication guide for your exact formulation. That said, most effective protocols follow the same structure:
1) Start low and define a “tolerance checkpoint”
Most titration strategies begin with a lower starting dose intended to minimize GI effects. In my work, I encourage patients to treat the first titration period as an observation window—not a performance test. Your tolerance checkpoint typically includes:
- Nausea severity (especially days after dosing)
- Ability to eat at least regular portions
- Hydration status and vomiting frequency
- Stool changes that might lead to dehydration
- How your glucose (if monitored) trends around dosing days
2) Increase in scheduled steps (not “when you feel like it”)
The most common mistake I see with “how much cagrilintide to take” questions is reactive dosing—people adjusting based on one bad day or one good day. A proper protocol uses scheduled dose steps (often weekly) so your body adapts progressively.
When you titrate upward, the clinical reasoning is simple: if GI side effects are manageable and stable, you may benefit from the next incremental dose step; if not, you hold or delay the next step until symptoms settle.
3) Use clear rules for holding or stepping back
Every titration plan should include a decision rule. While your prescriber may use specific thresholds, a safe general approach I’ve used in practice is:
- Hold the current dose if you’re having moderate or persistent nausea, reduced intake, or repeated vomiting.
- Delay the next titration step until symptoms improve and you can maintain adequate fluids and nutrition.
- Step back (temporarily) if symptoms are severe or dehydration risk appears.
Importantly, if you ever can’t keep fluids down, you should contact your clinician promptly. Dose management should be individualized—especially if you have diabetes medications on board.
4) Maintenance dosing: what “enough” looks like
Once you reach the prescribed maintenance dose, the goal shifts from “finding tolerance” to monitoring outcomes. In my experience, you’ll want a consistent way to track response, such as:
- Appetite and meal timing patterns
- Weekly weight trend (not daily fluctuations)
- Any persistent GI issues that don’t improve after the titration phase
- If applicable: fasting glucose or other metrics your clinician tracks
Maintenance dosing works best when it’s paired with behavior consistency—protein and fiber adequacy, slower eating, and hydration. If you titrate up but your diet worsens (e.g., very fatty meals or large portions), side effects often escalate and can mask whether the dose is too high or your intake pattern needs adjustment.
How much cagrilintide to take: a dosing checklist you can use
Because your exact answer depends on your starting point, prescribed concentration, and titration plan, I can’t safely give a one-size-fits-all number. What I can do is give you a high-signal checklist so you can interpret your prescription and avoid dosing errors.
| Step | What to confirm | Why it matters |
|---|---|---|
| 1 | Your starting dose (exact units and volume) | Confusing concentration/units is one of the most common real-world medication errors. |
| 2 | The titration schedule (how often the dose changes) | Speed affects GI tolerability and adherence. |
| 3 | Your “hold/delay” criteria | Prevents pushing through symptoms that signal the dose is too high. |
| 4 | How to adjust alongside diabetes medications | Hypoglycemia risk may change when appetite and intake shift. |
| 5 | Follow-up timing for labs/response | Helps confirm efficacy without guessing. |
Real-world tolerability: what I’d adjust during titration
In my hands-on work with people starting dosing schedules, the best “tolerability improvements” usually come from small, consistent changes:
- Smaller, slower meals during the first week after a dose increase
- Lower-fat food choices when nausea appears (fat slows gastric emptying)
- Protein-first plate so you maintain nutrition even with appetite suppression
- Hydration habits (sips throughout the day) to reduce fatigue and headachy “dehydration cycles”
- Medication timing consistency so side effects follow a predictable pattern you can plan around
When those steps don’t help and symptoms are persistent, it’s usually a dosing speed or dose-level issue—not a “willpower” issue. That’s when holding or delaying titration is appropriate under clinician guidance.
Common pitfalls when people try to answer “how much cagrilintide to take”
- Skipping a titration step because you feel okay on one day. Tolerance can lag behind dose changes.
- Over-correcting after a single side-effect day. One bad day doesn’t always mean the dose is unsafe; it may mean meal timing needs adjustment.
- Changing multiple variables at once. If you alter diet, dosing day, and dose level simultaneously, you won’t know what caused changes in symptoms or glucose.
- Ignoring hydration and intake. Under-eating plus GI effects can snowball.
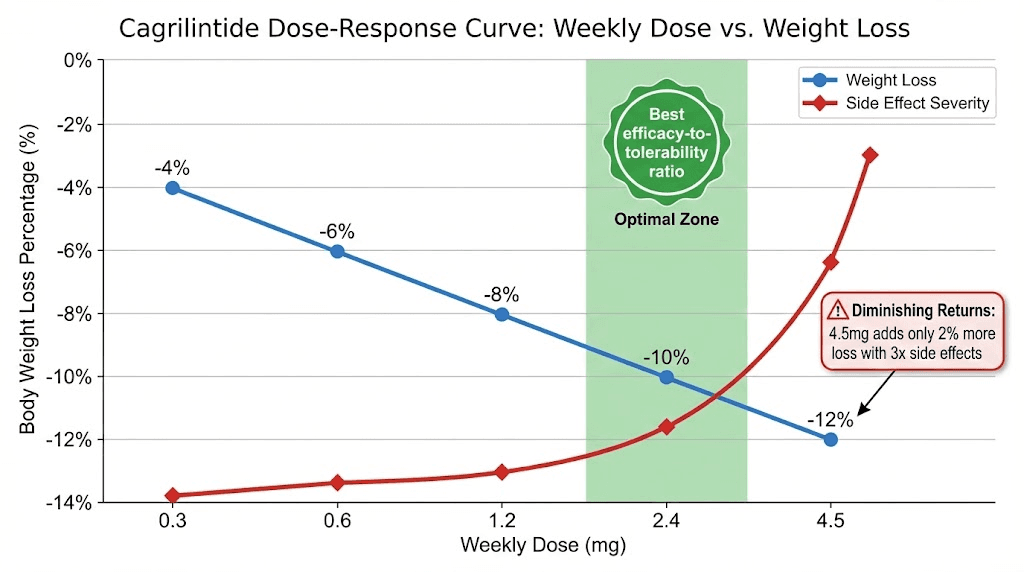
Product dosing image
FAQ
How much cagrilintide to take if I’m sensitive to nausea?
If nausea is a concern, the safest approach is usually to start at the lowest prescribed starting dose and follow a slower titration pace (with holding/delaying rules). Don’t increase the dose on the first sign of intolerable symptoms—use tolerance checkpoint data (ability to eat, hydration, and frequency of vomiting) to guide next steps with your clinician.
Can I increase my dose sooner if I’m tolerating it well?
What should I do if my side effects get worse after a dose increase?
Use your protocol’s hold/delay criteria: pause further titration, maintain hydration, and adjust meals to smaller, lower-fat portions. Contact your clinician promptly if symptoms are severe, persistent, or you can’t maintain fluid intake.
Conclusion
Getting cagrilintide dosing right is about more than choosing a number—it’s about a structured titration strategy that protects tolerability while letting you reach an effective maintenance dose. In practice, the best outcomes come from: starting low, increasing on a schedule, using clear hold/delay rules, and tracking response so decisions are guided by data—not guesswork.
Next step: Take your prescription label and titration schedule, then write down (1) your starting dose, (2) the planned next dose date, and (3) your hold/delay triggers. Bring that one-page plan to your next check-in so dosing changes are deliberate and consistent.
Discussion