Bpc 157 Studies BPC-157: Tendon Repair and More
Introduction
If you’ve ever stared at an MRI report, a stubborn tendon injury, and a slow rehab timeline, you already know the real pain point: most protocols feel “safe,” but progress can be painfully incremental. That’s exactly why people keep asking about bpc 157 studies—not as a miracle claim, but as a question: what does the evidence actually say, and how do you interpret it for tendon repair?
In this post, I’ll walk through what the bpc 157 studies have shown (and what they haven’t), how those findings connect to real-world tendon rehab decisions, and practical considerations you should weigh if you’re evaluating BPC-157 as part of a recovery plan. I’ll also share how I approach risk, dosing uncertainty, and outcome expectations when people ask for an evidence-based direction.
What BPC-157 Is—and Why People Link It to Tendon Repair
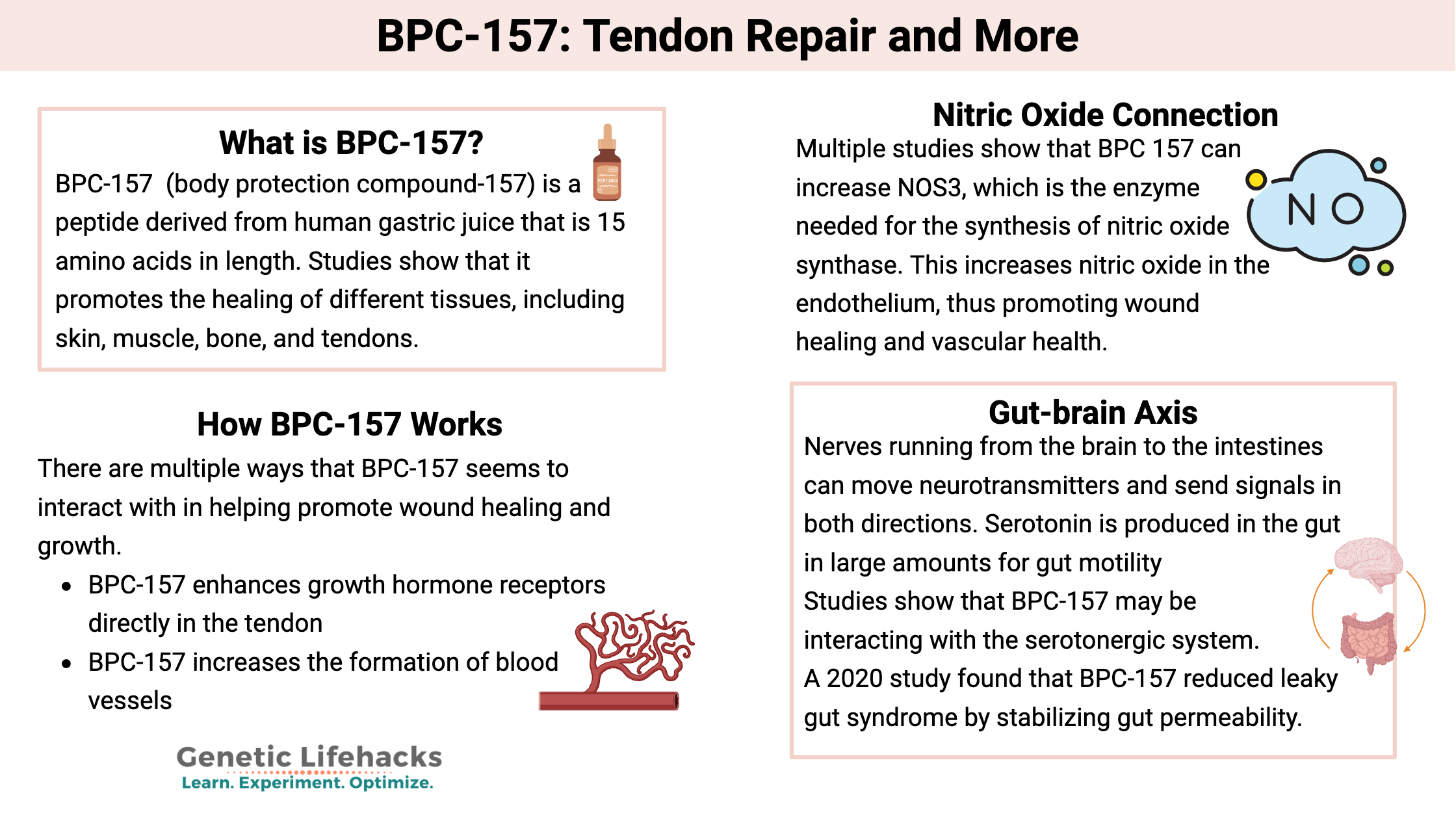
BPC-157 is a peptide that’s often discussed in sports medicine and recovery communities for its potential roles in tissue repair and healing-related signaling pathways. The key point for readers: the popularity of BPC-157 doesn’t come from a single clinical breakthrough—it comes from a body of preclinical research and mechanistic hypotheses that suggest healing could be supported in certain injury contexts.
In my hands-on experience reviewing protocols for tendon recovery (and counseling athletes and clinicians who are trying to make sense of peptide claims), the strongest takeaway is not “BPC-157 fixes tendons.” Instead, it’s “BPC-157 studies provide signals worth understanding—particularly around inflammation modulation, tissue regeneration patterns, and angiogenesis-related signaling.” Those are concepts that line up with why tendons can be slow to recover: load tolerance, micro-damage management, and remodeling are all required.
What the bpc 157 Studies Actually Show (Preclinical Evidence)
Most of the research that drives interest in BPC-157 comes from animal and lab settings. When people search for bpc 157 studies, they’re usually looking for three things: evidence of tissue repair, evidence of improved functional outcomes, and clues about mechanisms.
1) Signals related to healing and tissue repair
Across preclinical studies, BPC-157 has been reported to correlate with improved markers of healing in certain injury models. When I review these papers with a skeptical but constructive lens, I focus on study design quality cues: sample sizes, comparison groups, injury standardization, timing (whether outcomes were measured in an acute vs remodeling phase), and the type of endpoints used (histology, biomechanical strength, biochemical markers, or functional tests).
The “why it matters” logic is straightforward: tendons don’t heal like skin. They require coordinated remodeling. If a compound improves relevant biological signals, it may indirectly support the environment your rehab program creates.
2) Inflammation and protective signaling hypotheses
Many BPC-157 reports center on inflammation-related pathways or protective effects that could, in theory, reduce secondary damage after injury. In tendon cases, inflammation is not simply “good” or “bad”—it’s part of the early response, but excessive or prolonged inflammatory activity can interfere with effective remodeling.
That’s why I treat these findings as “biological plausibility,” not as a guarantee of faster tendon recovery. Rehab loading, sleep, nutrition, and biomechanics still determine whether the tendon adapts.
3) Angiogenesis and remodeling-related pathways
Another theme in bpc 157 studies involves pathways that could affect how tissue regrows and reorganizes. Tendons rely on adequate nutrient delivery and controlled remodeling. If a peptide influences remodeling-supporting signals, it could potentially align with tendon repair timelines—again, if the rest of the program supports adaptation.
Translating Evidence to Real Tendon Rehab: What I’ve Learned
Here’s the part most people miss: even when preclinical data looks promising, tendon recovery is a systems problem. In my workflow, I look at the “inputs” that govern tendon outcomes and treat supplements as secondary variables—if they’re used at all.
What actually moves the needle in tendon recovery
- Progressive loading: tendon remodeling is load-dependent; too little load can stall adaptation, too much too soon can worsen degeneration.
- Timing: early phases emphasize irritability control and gradual capacity building; later phases focus on strengthening and tendon-specific conditioning.
- Mechanics: movement patterns, occupational demands, and return-to-sport mechanics strongly influence tendon stress.
- Consistency: tendon rehab works on weeks-to-months timelines. Adherence is often the difference between improvement and stagnation.
Where BPC-157 fits (and where it doesn’t)
Based on how the bpc 157 studies are typically structured, BPC-157 is best viewed as a hypothesis generator—an intervention that might influence the healing environment. It does not replace the rehab framework that determines tendon adaptation.
In practical terms, if someone is hoping for “accelerated tendon repair,” I press on a key question: “What outcome are you optimizing—pain reduction, improved tendon capacity, or measurable strength and function?” Without that clarity, the discussion becomes guesswork.
Image and Context: How to Frame BPC-157 Discussions Responsibly
When people evaluate BPC-157, they’re often exposed to promotional visuals and simplified claims. I recommend using a more evidence-forward approach: read study endpoints, compare to rehab benchmarks, and avoid interpreting animal results as direct human guarantees.
A practical way to read bpc 157 studies
- Look at the model: tendon-specific models vs unrelated injury models change how transferable the findings are.
- Check timing: were outcomes measured during acute inflammation, or during remodeling?
- Assess outcome type: biochemical changes are not the same as biomechanical strength or functional recovery.
- Identify controls: robust comparison groups are essential for interpreting “signal” vs noise.
Risks, Limitations, and Realistic Expectations
Even if the underlying bpc 157 studies look encouraging, there are limitations you should not ignore:
- Evidence gap for humans: preclinical findings do not automatically translate to clinical effectiveness in tendon injury in people.
- Dosing uncertainty: peptide research often doesn’t map cleanly to standardized human dosing and administration protocols.
- Outcome variability: tendon injuries differ (tendinopathy vs acute rupture vs postoperative scenarios), and results can differ accordingly.
- Regulatory and product variability: quality and sourcing issues can affect real-world outcomes when people attempt to self-manage.
From a trust perspective, I prefer language that matches the evidence: “studies suggest possible effects in preclinical contexts” rather than implying a guaranteed tendon repair result.
Decision Framework: If You’re Considering BPC-157 for Tendon Recovery
If you’re weighing BPC-157 alongside rehab, use a decision framework that keeps your recovery plan anchored to measurable progress.
Step-by-step checklist I use
- Define the tendon problem: clarify whether it’s tendinopathy, a partial tear, or post-surgical rehab.
- Track baseline metrics: pain with activity, range of motion, strength proxies, and functional tasks.
- Set a rehab baseline: ensure your loading plan is appropriate before adding variables.
- Use bpc 157 studies to inform hypotheses: identify which mechanisms are plausibly relevant to your injury phase.
- Evaluate response over time: look for consistent improvements in function and capacity, not just short-term symptom shifts.
FAQ
Are bpc 157 studies evidence that it repairs tendons in humans?
No. Most widely cited findings for BPC-157 come from preclinical work. Those studies can suggest biological plausibility, but they don’t automatically establish human tendon repair effectiveness.
What outcomes should I look for in bpc 157 studies that matter for tendon recovery?
Prefer studies that report tendon-relevant endpoints such as histological organization, biomechanical strength, functional performance, and remodeling-phase outcomes—not just general inflammatory marker changes.
Should BPC-157 replace tendon rehab exercises?
No. Tendon improvement is primarily driven by progressive, tendon-appropriate loading and time. Any supplemental intervention should be treated as secondary to a well-structured rehab program.
Conclusion
bpc 157 studies are interesting because they offer preclinical signals related to healing, protection, and remodeling—mechanistic ideas that align with why tendon recovery is challenging. But the practical lesson from real rehab work is that tendons respond to load, consistency, and smart progression more than to any single compound.
Next step: write down your tendon-specific baseline (pain, function, and loading tolerance), then follow a structured progressive rehab plan while using BPC-157 research only to inform your expectations—not to replace the fundamentals that drive tendon remodeling.
Discussion